
Sina Salavati1, Muhammad H Kafrashi2, Daryoush Babazadeh3*, Mohammadreza Raznahan2
- Department of Small Animal Medicine, Faculty of Veterinary Medicine, Shiraz University, Shiraz, Iran
- Faculty of Veterinary Medicine, Ferdowsi University of Mashhad, Mashhad, Iran
- Pet and Exotic Diseases Clinic, Aria Veterinary Hospital, Mashhad, Iran
* Corresponding author: Daryoush Babazadeh, School of Veterinary Medicine, Shiraz University, Shiraz, Iran. Email: daryoush.babazadeh@shirazu.ac.ir
ABSTRACT
Introduction: Fibrocartilaginous embolic myelopathy is a non-progressive injury in the spinal cord that can cause infarction in veins of spinal parenchyma which leads to ischemia and necrosis.
Case report: Fibrocartilaginous embolic myelopathy was diagnosed in a 4-year-old, female, Spitz dog using the clinical neurological examination. The dog was hospitalized, and the treatment including supportive treatment and Cortone was set up for three weeks. Then Diazepam and Methocarbamol were added to the prescription and treatment continued for two weeks. A general improvement was noted after three weeks, and the dog could stand perfectly after 5 weeks.
Conclusion: Three weeks of supportive treatment, Cortone therapy as well as the addition of Diazepam and Methocarbamol to the treatment could help the dog to stand on its feet. However, cannot be ignored that knowing about the history of the dog played an important role in its treatment procedure.
Keywords: Cortone, Dog, Fibrocartilaginous embolic myelopathy, Spinal Cord
1. Introduction
Fibrocartilaginous embolic myelopathy is an acute and non-progressive injury in the spinal cord that spinal materials, such as fibrous and cartilage cause infarction in arteries and veins of spinal parenchyma followed by ischemia and necrosis1. In the initiation of the disease, pain exists but in clinical examination, the dog has no signs of pain which can be differentiated with disc hernia type 1, spinal fractions, and luxation of the vertebra2. The patient suddenly becomes paraparesis3.
2. Case Report
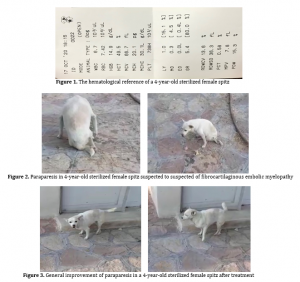
In October 2020, a 4-year-old sterilized female spitz was referred to the Aria Veterinary Hospital, Mashhad, Iran. the owner’s complication was that the dog suddenly became disabled to walk on her back legs last night without any history of trauma. During the clinical and physical examination, the dog was quite alert indicating paraparesis, perineal hyperreflexia, colonic patellar reflex, negative panniculus reflex, normal hopping and knuckling reflex in hands, hypertonia, and stiff muscle in hands on the lateral position as well as mild hypotonia and no deep pain in legs. The hematological reference ranges and the radiographs were also normal (Figure 1, radiographs are not archived).
According to the clinical neurological examination and the history, the animal was suspected of Fibrocartilaginous Embolic Myelopathy (FCE) from T3 to L3 (Figure 2). The dog was hospitalized, and the treatment including supportive treatment (fluid therapy for 5-6% dehydration, 10 ml of Duphalyte q12h, etc,.) and Cortone (prednisolone at the dose of 1.1 mg/kg, tapper off) was set up for two weeks. Then the owner of the dog decided to change the veterinarian, and the second veterinarian added Diazepam and Methocarbamol to its prescription for a week. After 5 weeks the dog could stand perfectly (Figure 3).
3. Discussion
Spinal cartilage fibrosis embolism is a severe spinal lesion, and can be observed in animals aged an average of three to seven years with any history of trauma or heavy activities4. Cerebrospinal Fluid, Magnetic Resonance Imaging (MRI), Computerized Tomography (CT) scan may be usually normal in these patients5. Symptoms depend on the location and severity of the spinal cord injury6. The lesions occur mainly in the thoracolumbar (T3-L3) and lumbosacral (L4-S3) regions. In T3-L3 spinal cord injuries, the hands are expected to be normal, but the legs show Upper Motor Neuron (UMN) signs1,7. However, in severe injuries to this area, when the animal lies on its sides, the hands dilate due to the nerve amputation of ascending inhibitory axons originating from the cells of the spinal cord located in sections L1-L7 (Schiff Sherrington syndrome)1. The Lower Motor Neuron (LMN) symptoms in the legs can indicate spinal shock in the area8.
According to the references, treatment for FCE includes
nonspecific supportive measures, physiotherapy, and nursing care. For the animals brought to the medical hospitals during the first six hours, methylprednisolone sodium succinate can be suggested aggressively (as a treatment of acute spinal cord trauma)1,7. While corticosteroids can be used for the treatment of FCE (at the anti-inflammatory doses), intensive interventions with physiotherapy are needed to hinder the bedsores and urinary tract infections2.
In the present case report, although Diazepam and Methocarbamol were thought to be the key point of treatment after they were added to the protocol, they are not specifically mentioned for the treatment of FCE in any available references. On the other hand, most clinical improvements usually occur within seven to 10 days after the onset of clinical signs (even it may take six to eight weeks for a complete rehabilitation). Therefore, more investigations in a larger sample size with an exact statistical analysis are required to prove the role of Diazepam and Methocarbamol in the improvement of the lesions of FCE.
4. Conclusion
Fibrocartilaginous embolic myelopathy is an acute disease in patients; history is very helpful for diagnose. The disease is usually self-limited and nonspecific supportive measures, and nursing care and corticosteroids are useful. Effect of Drugs like Diazepam and Methocarbamol for such patients required to prove the role.
Declarations
Competing interests
Authors declare no conflicts of interest.
Authors’ contribution
Sina Salavati, Muhammad H Kafrashi, and Mohammadreza Raznahan diagnosed the case and conducted the treatment. Daryoush Babazadeh supervised the whole procedure.
Acknowledgments
Authors would like to express their gratitude to Aria Veterinary Hospital, Mashhad, Iran.
References
- de Lahunta A, Glass E, Kent M. Veterinary neuroanatomy and clinical neurology.4th St. Louis: Saunders. 2015; p. 268-262. Available at: https://www.elsevier.com/books/veterinary-neuroanatomy-and-clinical-neurology/de-lahunta/978-1-4557-4856-3
- Nelson RW, Couto CG. Neuromuscular Disorders. Small Animal Internal Medicine. 5 ed. St. Louis: Mosby: 2019; p. 1059-1060.
- Ettinger S, Feldman E, Cote E. Veterinary Internal Medicine,
Elsevier, 8th 2017; p. 3478-3481. Available at: https://www.elsevier.com/books/textbook-of-veterinary-internal-medicine-expert-consult/ettinger/978-1-4557-3633-1 - Cauznille L, Kornegay JN. Fibrocartilaginous embolism of the spinal cord in dogs: Review of 36 histologically confirmed cases and retrospective study of 26 suspected cases. J Vet Intern Med. 1996; 10: 241-245. Available at: https://pubmed.ncbi.nlm.nih.gov/8819049/
- Sarchahi AA. Neurological examination and nervous system disorders of small animals, 2nd 2016; p. 353-355.
- Smith PM, Jeffrey ND. Spinal shock-comparative aspects and clinical relevance. J Vet Intern Med. 2005; 19: 788-793. Available at: https://pubmed.ncbi.nlm.nih.gov/16355670/
- de Lahunta A, Alexander JW. Ischemic myelopathy secondary to presumed fibrocartilaginous embolism in nine dogs. J Am Anim Hosp Assoc. 1976; 12: 37. Available at: https://agris.fao.org/agris-search/search.do?recordID=US19770151858
- Simpson RK, Robertson CS, Goodman JC. Glycine: An important potential component of spinal shock. Neurochem Res. 1993 Aug; 18: 887-892. Available at: https://pubmed.ncbi.nlm.nih.gov/8103919/
